Behavioral Health Insurance Eligibility & Benefits Verification Automation: Stop Denials Before They Happen
- 5 hours ago
- 7 min read

Most denied behavioral health claims were lost before the visit even happened. The patient's coverage had lapsed, the plan didn't cover that level of care, the copay was wrong, or a prior authorization was required and nobody got it — all knowable at the front desk, all missed because verifying insurance is slow, manual, and the staff are buried. By the time the denial comes back weeks later, the work is done, the revenue is at risk, and someone has to fight to recover it. Automating eligibility and benefits verification is how a behavioral health provider moves that check to the front — and it's one of the clearest software and integration wins in the entire revenue cycle.
Eligibility errors cause 27% of claim denials — and up to 65% of denied claims are never reworked. That's revenue you earned, lost to a coverage check that takes software seconds and a human ten minutes nobody had.
Behavioral health insurance eligibility and benefits verification automation uses software to check a patient's coverage, benefits, copays, and prior-authorization requirements in real time — before the appointment and before the claim — so the issues that cause denials get caught and fixed at the front end instead of weeks later in appeals. This guide covers why most denials are preventable, what automation changes, and when to build it.
Why are most behavioral health denials preventable?
Because the leading causes of denial are front-end problems — coverage and authorization — not clinical ones. Studies find that eligibility errors cause about 27% of claim denials, and 35–60% of all denials relate to eligibility and authorization issues (Practolytics). More than a quarter of providers say at least 10% of their denials trace back to inaccurate or incomplete data collected at intake. These aren't tricky medical-necessity disputes; they're "we didn't check, or checked wrong" problems — exactly what software catches.
Behavioral health has it worse than most. Behavioral health claims rose 17% in 2025, and that utilization surge has accelerated payer scrutiny, with prior-authorization denials for residential and PHP/IOP levels of care now the leading RCM challenge heading into 2026. The combination — more claims, stricter payers, and a sector still running on manual processes — is a denial machine. Front-end verification automation is the most direct way to jam it.
What does getting it wrong actually cost?
A fortune, most of it invisible. Every denied claim costs $25 to $118 to rework, and up to 65% of denied claims are never reworked at all — that's pure lost revenue (Practolytics). Across the industry, the American Hospital Association estimates providers spend nearly $20 billion a year reprocessing denied claims. And the problem is getting worse: 41% of providers now report denial rates of 10% or higher, a number that's climbed every year since 2022.
Run that math for a behavioral health practice. A denial you rework costs staff time you're already short on; a denial you don't rework — the majority — is revenue you earned and simply lost. Front-end verification flips the economics: catching a coverage or authorization problem before the visit costs almost nothing, while catching it after the claim costs $25–118 if you're lucky and the full claim value if you're not. The cheapest denial is the one that never happens.
What does the automated verification flow look like?
The whole idea is to move the check upstream — to verify before the encounter, not discover after the claim.
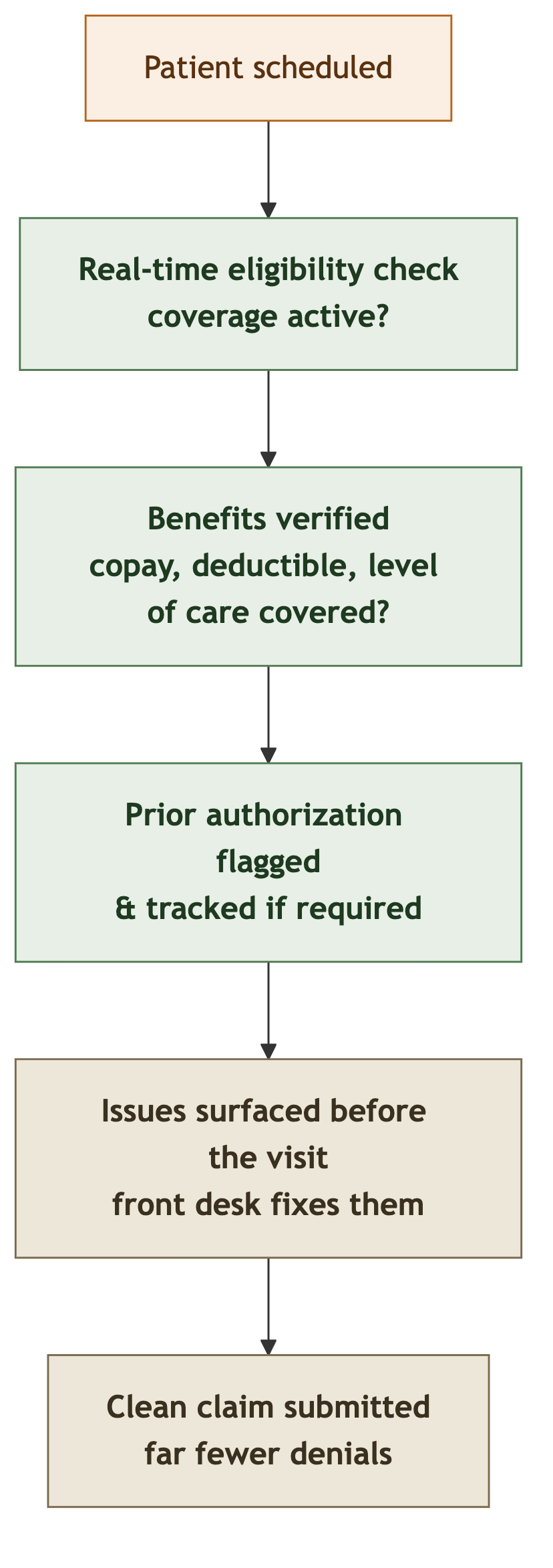
When this runs, the front desk knows before the patient walks in whether coverage is active, what the patient owes, whether the level of care is covered, and whether a prior auth is needed — and can fix any problem while it's still cheap to fix. The denial that would have cost $118 and a three-week appeal becomes a thirty-second correction at scheduling. That upstream shift is the entire value.
What does good verification automation actually do?
Judge any solution against the front-end work it removes:
Real-time eligibility checks — confirm active coverage automatically at scheduling and again before the visit, not by a staffer on hold with the payer.
Benefits verification (VOB) — surface copay, deductible, out-of-pocket status, and whether the specific level of care is covered.
Prior-authorization tracking — flag when an auth is required, and track its status so a residential or IOP admission isn't billed without it.
Denial-pattern detection — learn from past denials to flag at-risk claims before they're submitted.
Integration with the EHR and billing — verification results land in the chart and the billing system, so nobody re-keys and nothing is missed.
That last point is what separates a real solution from a standalone tool: verification only prevents denials if its results actually reach the people and systems making the claim. That makes it a systems integration job as much as an automation one.
Drowning in eligibility and prior-auth denials you could have caught up front? Book a free consultation and we'll map your front-end verification process, find where preventable denials originate, and tell you honestly whether an RCM tool or a custom integration into your EHR fits. No obligation.
Build, buy RCM software, or integrate?
Most behavioral health practices should start with RCM software that includes verification — and several behavioral-health-specific platforms do exactly this. If one fits your EHR and your payers, use it. The custom or integration case appears when the packaged tools don't reach your reality:
Your EHR doesn't connect to the verification tool, so results don't flow into the chart and billing without re-keying.
Behavioral-health-specific payer rules — level-of-care authorizations and carve-outs the generic tool doesn't model.
A multi-location or multi-payer operation where verification has to span systems no single tool unifies.
You want denial-pattern detection tuned to your historical denials, not a generic model.
If a packaged RCM tool fits, use it; building would be waste. If verification has to integrate with your specific EHR and payer mix to actually prevent denials, that's a focused custom integration, and the same custom-versus-off-the-shelf judgment applies. We've seen how often the real problem in behavioral health isn't the tool but the data and integration underneath it.
What about prior authorization specifically?
Prior authorization deserves its own attention, because it's where behavioral health denials concentrate hardest. Unlike a general office visit, the higher levels of behavioral health care — residential, partial hospitalization (PHP), and intensive outpatient (IOP) — almost always require payer authorization before services are rendered, and payers have been tightening that scrutiny as utilization climbs. A residential admission billed without a completed auth isn't a partial denial; it's often a total loss on a high-dollar claim.
Manual prior-auth management is where this breaks down: an auth gets requested but not tracked, expires mid-stay, or covers fewer days than the patient actually needs, and nobody notices until the claim bounces. Automation makes the requirement visible and the status trackable — flagging at scheduling that an auth is needed, tracking its approval and expiration, and alerting staff before an authorization lapses during an active episode of care. For providers offering residential or IOP/PHP services, this single capability often justifies the whole verification automation effort, because the claims at stake are the largest in the practice. It's also why generic eligibility tools fall short for behavioral health: they verify coverage but don't model the level-of-care authorization logic that drives the sector's biggest denials, which is exactly where custom rules and integration earn their place.
A worked example: the denials that never should have happened
Take a behavioral health practice with a denial rate creeping past 12%. Most denials cluster in two buckets: coverage that had lapsed or didn't cover the service, and IOP admissions billed without a completed prior authorization. The front desk verifies insurance manually when they can, but they're short-staffed, so checks get skipped under load — and every skipped check is a future denial. Billing spends its days appealing problems that were knowable weeks earlier.
The fix is front-end automation integrated with the EHR: every scheduled patient gets an automatic real-time eligibility check; benefits and level-of-care coverage are verified and written to the chart; prior-auth requirements are flagged and tracked so no IOP admission proceeds unauthorized; and any issue surfaces to the front desk before the visit. The denial rate falls back toward benchmark, billing stops fighting preventable appeals, and the revenue that was quietly leaking through the 65% of never-reworked denials comes back. Nothing about the care changed — the practice just stopped submitting claims it already knew would be denied. That's the pattern: verify upstream, integrate the result, and prevent the denial instead of appealing it.
What does it cost, and how should you start?
Start by measuring your denial rate and categorizing your denials — what share are eligibility, benefits, and prior-auth problems versus genuine medical-necessity disputes. For most behavioral health practices, the front-end bucket is the majority, and that number sizes the opportunity directly: every preventable denial is $25–118 of rework plus the majority you never recover. If your RCM software's verification reaches your EHR and payers, it's a modest subscription and the right first move. If verification has to be integrated with your specific systems and payer rules to actually work, a custom integration is a bounded build that pays back fast against denial recovery. The honest sequence is: categorize the denials, check whether a packaged tool prevents them, and integrate or build where your EHR and payers are specific — which we scope in a no-risk discovery.
The bottom line
Behavioral health insurance eligibility and benefits verification automation prevents the denials that cause most of a practice's lost revenue — the coverage, benefits, and prior-authorization problems that are knowable at the front desk and cause 35–60% of denials. By moving the check upstream and integrating the result into the EHR and billing, it turns a $118 appeal into a thirty-second correction and recovers the revenue lost to the 65% of denials never reworked. Buy behavioral-health RCM software if its verification reaches your systems; build a custom integration when your EHR and payer rules are specific. Either way, the cheapest denial is the one that never happens. If your denial rate is climbing, categorizing those denials is worth doing before the next billing cycle.
By the CodeStringers Team — Zoho Experts & Custom Software. CodeStringers is a custom software engineering firm that builds and integrates secure, compliance-sensitive systems for healthcare and behavioral health providers, writing from work we've actually shipped. [Book a free consultation.](/how-we-work/no-risk-discovery)

































Comments